AI in Clinical Research: What It Really Means in 2026
By Rajesh K Singh · Reviewed July 2026
Two stories about AI keep circulating in clinical research, and both are wrong.
The first says AI will soon run trials end to end — recruiting patients, cleaning data, writing submissions — and the people who do that work today should start worrying. The second says it is all hype, another wave of vendor slideware that will pass like blockchain did. If you hold a pharmacy or life-science degree and you are trying to plan a career around this field, neither story helps you. What helps is knowing what the technology actually does inside a trial right now, what it cannot do, and what regulators will and will not accept. That is what this article covers.
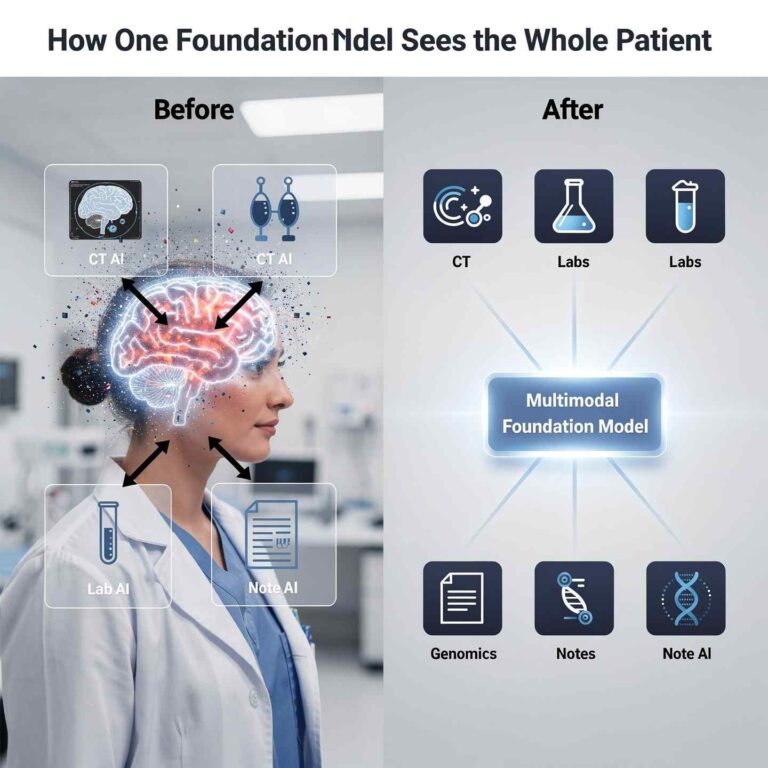
Start with a working definition. AI in clinical research is the use of software that learns patterns from data to support the design and conduct of clinical trials — finding eligible patients, flagging data errors, surfacing safety signals, and drafting documents — while qualified humans retain the scientific judgment and the legal responsibility for every decision. That last clause is not a courtesy to nervous professionals. It is how the entire system is built, and, as we will see, how regulators insist it stays built.
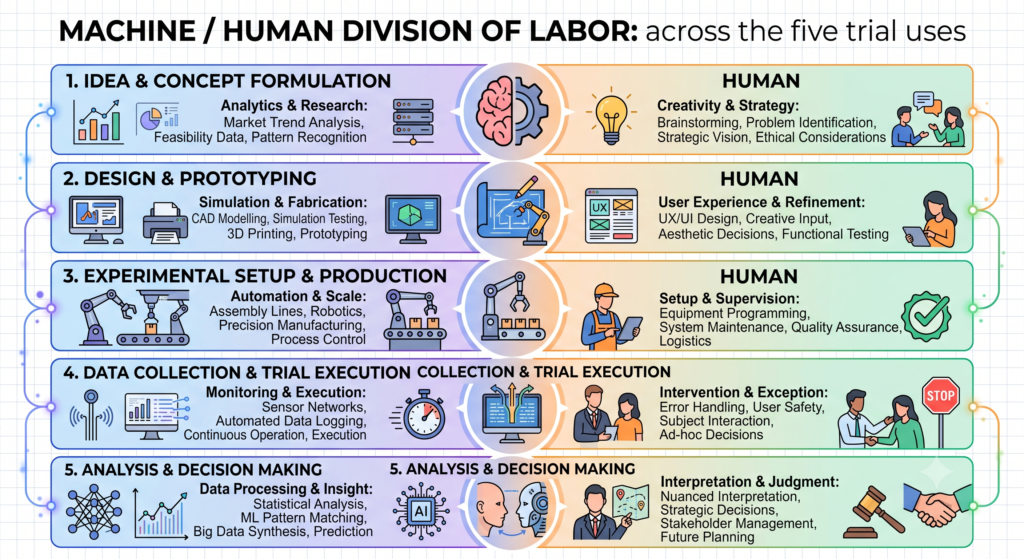
Across every established use of AI in trials, the machine takes the volume and the human keeps the judgment.
What the words actually mean
The field uses three terms that get blurred together, and the blur causes most of the confusion.
Artificial intelligence is the umbrella: software doing tasks that were once thought to need human judgment. Machine learning is the type of AI that dominates clinical research today — instead of following hand-written rules, it learns patterns from data. Show a machine-learning model thousands of past patient records and trial outcomes, and it learns what an eligible patient or a suspicious data point tends to look like. Generative AI — the large language models behind tools like ChatGPT — is the newest branch. Rather than only making predictions, it produces text: draft protocols, draft summaries, draft safety narratives.
The distinction matters in practice. Machine learning is the quiet workhorse that has been inside trial software for years. Generative AI is the loud newcomer that writes fluent first drafts and, as we will get to, sometimes fluent fiction. They carry different risks and demand different kinds of human oversight.
Why this stopped being optional in 2026
For years, a working professional could reasonably ignore AI. The evidence says that window has closed.
The clearest signal comes not from vendors but from the regulator’s inbox. The FDA’s drug-review centre, CDER, has reported experience with more than 500 drug and biologic submissions containing AI components since 2016, concentrated in areas such as oncology and neurology. Those are not pilots or press releases. They are real regulatory submissions for real medicines, and their number tells you that pharmaceutical companies and contract research organisations (CROs) have already moved.
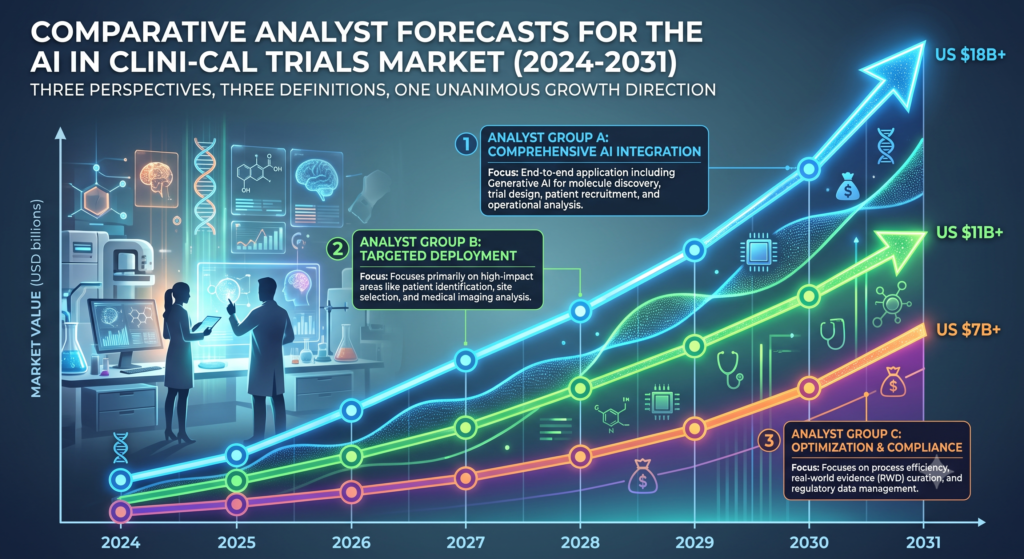
The money tells the same story, though less precisely than the headlines suggest. Market analysts disagree sharply on how big the AI-in-clinical-trials market is, and the disagreement is worth pausing on. MarketsandMarkets sizes it at roughly USD 1.35 billion in 2024, forecast to reach about USD 2.75 billion by 2030 — around 12.5% annual growth. Mordor Intelligence puts it at roughly USD 2.68 billion in 2026, forecast to reach about USD 8.24 billion by 2031, growing near 25% a year. Beroe estimates roughly USD 2.7 billion in 2025, forecast to reach about USD 8.5 billion by 2030, at 24–28% annual growth.
The estimates differ by more than double because each analyst draws the boundary of “the market” differently — some count only trial-specific AI software, others fold in adjacent services. Treat every one of these numbers as a forecast, not a fact. What they agree on is direction: fast growth, driven by pharma companies and CROs putting AI into how trials are actually run. When independent analysts using different definitions all point the same way, the direction is the reliable part.
How is AI used in clinical trials?
Here is the honest map. Across every established use, the same division of labour appears: the machine takes the volume, the human keeps the judgment. It shows up so consistently that once you see it, you can predict how any new AI tool in this field will be deployed.
Patient recruitment and matching
Finding eligible patients is the costliest bottleneck in clinical research — trials stall, sites sit idle, and budgets bleed while coordinators hunt for people who meet the protocol’s criteria. AI attacks this directly. Models read through electronic health records and match patients against eligibility criteria far faster than any human could page through charts. This is the most established and least-disputed application of artificial intelligence in clinical trials, precisely because the bottleneck it addresses is so expensive. But the model only proposes. A human confirms eligibility, handles informed consent, and has the conversation with the patient. No algorithm consents anyone into a trial.
Trial design
Before a trial ever recruits its first patient, someone has to design it — endpoints, sample size, inclusion criteria, duration. Machine learning models trained on data from past trials can suggest protocols and endpoints that are realistic rather than optimistic: designs less likely to fail for reasons that historical data could have predicted. The scientist still owns the science. A human team weighs the suggestions, applies clinical knowledge the model does not have, and approves the final design.
Clinical data management
Trial data arrives messy — transcription slips, impossible values, patterns that suggest a site is doing something wrong. AI models flag anomalies and likely errors early, when they are cheap to fix, instead of surfacing at database lock, when they are expensive and embarrassing. A human data manager investigates each flag and resolves it, because a flag is a suspicion, not a verdict. This area is deep enough to deserve its own treatment, which you can find in our article on AI in clinical data management.
Pharmacovigilance
Drug-safety teams face a volume problem: individual case safety reports arrive by the tens of thousands, and a genuine safety signal can hide inside the noise. AI sifts that volume and surfaces the cases and patterns most likely to matter — this is signal detection at machine scale. But causality — deciding whether a drug actually caused a harm — remains a human scientific judgment, and the final call always belongs to a qualified professional. The full picture is in our article on AI in pharmacovigilance.
Medical writing
Generative AI now drafts first versions of clinical documents: protocols, study summaries, safety narratives. A capable model can produce in minutes a draft that once took days. Then the human work begins — a qualified medical writer edits, verifies every factual claim against source data, and takes professional responsibility for the final document. Given what generative models can invent (more on that shortly), no serious organisation skips that step. We examine the workflow in detail in our article on AI in medical writing.
One table, because the pattern deserves to be seen whole:
|
Where AI works in a trial |
What the machine does | What the human keeps |
|---|---|---|
| Patient recruitment | Reads health records, matches patients to criteria | Confirms eligibility, obtains consent |
| Trial design | Suggests realistic protocols from past-trial data | Owns the science, approves the design |
| Data management | Flags anomalies and likely errors early | Investigates and resolves them |
| Pharmacovigilance | Surfaces possible safety signals from case reports | Judges causality, makes the call |
| Medical writing | Drafts first versions of documents | Edits, verifies, takes responsibility |
The honest limits
This is the part most articles skip, and it is the part you most need.
AI cannot guarantee its own output is correct. A model gives you an answer; it does not tell you whether the answer deserves your trust. Without deliberate validation — testing the model against cases where the truth is known — you have no way to know which outputs to rely on. This is why regulators talk about “credibility” rather than just accuracy: a model must be shown trustworthy for the specific job it is doing.
AI cannot replace clinical judgment or carry legal responsibility. When a decision about a patient or a drug goes wrong, a person answers for it. No framework anywhere transfers that accountability to software, and none is likely to.
AI is only as good as its training data. A model trained on narrow or biased data produces narrow or biased conclusions — and does so invisibly, with the same confident tone as a sound conclusion. In a field that decides which drugs reach which patients, that is not an academic worry. It is a patient-safety concern, and it is why questions about training data and bias sit at the centre of every serious model validation.
Generative AI hallucinates. Large language models can produce fluent, confident, entirely fabricated text — including citations formatted perfectly that refer to papers that do not exist. This single failure mode explains an industry-wide rule: no serious organisation lets generative AI write regulatory documents unsupervised. The technology drafts; a human verifies; the human signs.
None of these limits means the tools are useless. It means the tools are tools — and the professional who understands their failure modes is worth more than the one who only knows their features.
Is AI in clinical research regulated?
Yes — and 2025 was the year the answer became concrete rather than theoretical.
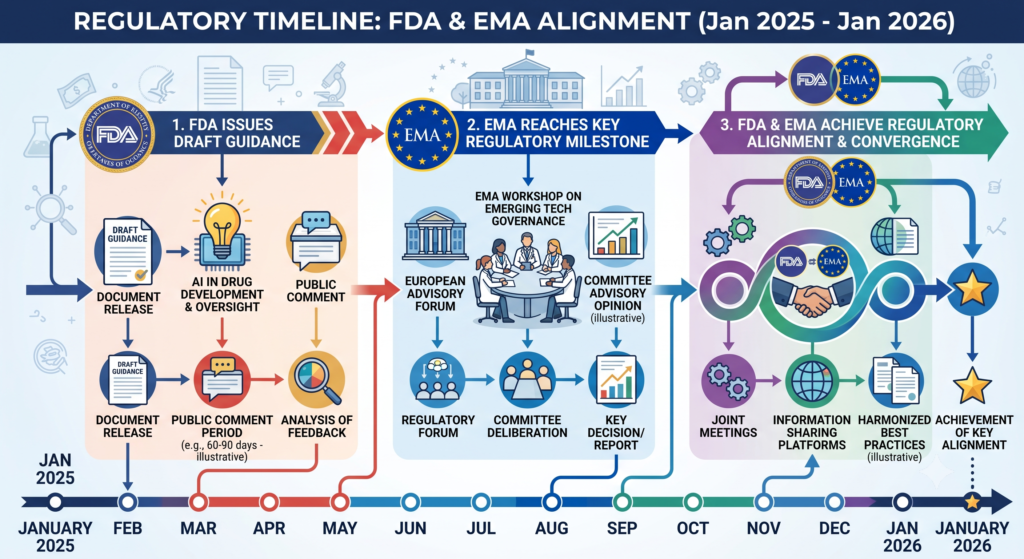
On 6 January 2025, the US FDA issued its first draft guidance on using artificial intelligence to support regulatory decision-making for drugs and biological products. Its core is a seven-step, risk-based credibility assessment framework, organised around an idea called Context of Use (COU): the specific job an AI model performs and how much its output influences a decision. A model whose output heavily shapes a high-stakes decision must clear a far higher evidence bar than one playing a minor supporting role. Notably, the guidance targets AI supporting decisions about a drug’s safety, effectiveness, or quality — it deliberately does not try to police every experimental use in early drug discovery. Regulate where the risk is; leave room to explore where it is not.
Europe moved in parallel. The European Medicines Agency (EMA) reached its first AI-model qualification milestone in March 2025. Then, in January 2026, the FDA and EMA aligned on shared principles for good AI practice in drug development — a meaningful step, because sponsors running global trials had feared having to satisfy two divergent rulebooks.
India, one of the world’s major hubs for clinical trials and clinical-research talent, is at an earlier stage. The CDSCO — the Central Drugs Standard Control Organisation, India’s national drug regulator — has not yet published a framework as detailed as the FDA’s; its approach is still evolving. What already applies is the Digital Personal Data Protection Act, 2023 (the DPDP Act), India’s data-privacy law, which governs how patient data may be collected and used. Anyone building or using AI on Indian patient data works inside that law today, whatever trial-specific rules follow.
The regulatory picture, in one sentence: the era of “AI in trials is a grey zone” is over, and the organising principle everywhere is risk-proportionate human oversight.
What this means for your career
Now the question you actually opened this article to answer.
For 2026, the evidence points one way: AI is augmenting clinical-research professionals, not replacing them. The roles that are genuinely shrinking are the purely manual ones — jobs that consisted mostly of moving and checking data by hand. The roles growing are the ones that combine clinical-research knowledge with the ability to use and judge AI tools: professionals who can read a model’s output and know when to trust it, question it, or overrule it. We take the replacement question apart properly in our article on whether AI will replace clinical research jobs.
The real divide forming in this field is not humans versus machines. It is professionals who can use AI versus professionals who cannot. That divide runs through pharmacovigilance teams, data-management groups, and medical-writing departments alike, and it will decide who gets hired for the interesting work.
So what should you actually learn? Two things. First, data literacy — enough understanding of how models work to interpret their output and, just as importantly, to intelligently distrust it. Second, judicious use of generative tools: drafting with them, verifying behind them, knowing where they break. What you do not need is to become a machine-learning engineer. Python genuinely helps in data-heavy roles such as clinical SAS programming and data management, but it is not required for many clinical-research jobs — we weigh the trade-offs in our article on whether you need Python. Understanding AI matters more than building it.
For readers who want a structured path rather than piecing this together alone, IICRS teaches exactly this combination — clinical-research fundamentals plus working AI skills — in its Advanced Diploma in AI in Clinical Research.

Where it is heading
Grounded expectations, plainly labelled. The regulatory direction is set: the FDA–EMA alignment of January 2026 suggests convergence, not fragmentation, and it is reasonable to expect other regulators — including India’s — to build on that foundation, though when and how remains genuinely uncertain. The commercial direction is set too: every credible forecast, whatever its numbers, points to more AI in trials, not less. What is speculative is the pace — whether decentralized trials, real-world evidence, and AI-assisted design compound each other quickly or slowly. Anyone who claims to know the timeline is selling something. For a longer look at the plausible paths, see our article on the future of AI in clinical research.
Frequently asked questions
How is AI used in clinical trials?
Five established ways: matching patients to trials by reading health records, suggesting realistic trial designs from past data, flagging errors in trial data early, surfacing possible drug-safety signals from case reports, and drafting clinical documents. In every case a qualified human reviews the output and makes the final decision.
Is AI in clinical research regulated?
Yes. The FDA issued draft guidance on 6 January 2025 built on a seven-step, risk-based credibility framework organised around “Context of Use.” The EMA reached its first AI-model qualification milestone in March 2025, and in January 2026 the FDA and EMA aligned on shared principles. India’s CDSCO framework is still evolving; the DPDP Act, 2023 governs patient data.
Will AI replace clinical research jobs?
Not in 2026. AI is augmenting professionals, not replacing them. Purely manual data-handling roles are shrinking, while roles combining clinical-research knowledge with the ability to use and judge AI tools are growing. The real divide is between professionals who can use AI and those who cannot.
Do you need Python for clinical research?
No — not for many roles. Python genuinely helps in data-heavy work such as clinical SAS and data management, but most clinical-research jobs need data literacy and sound judgment about AI outputs more than programming skill. Understanding AI matters more than building it.
What are examples of AI in clinical trials?
Models that read electronic health records to find eligible patients, machine learning that flags anomalies in trial data before database lock, systems that sift thousands of safety reports to surface possible signals, and generative AI that drafts protocols and safety narratives for human medical writers to verify.
What is AI in pharmacovigilance?
The use of AI to sift large volumes of individual case safety reports and surface possible safety signals for human review. The machine handles the volume; a qualified professional judges causality and makes the final safety call. It is one of the fastest-growing applications of AI in drug safety.
The essentials, in plain terms
- AI in clinical research means software that learns patterns from data to support trials — finding patients, flagging errors, surfacing safety signals, drafting documents — while humans keep the judgment and the legal responsibility.
- The FDA issued its first draft guidance on AI in regulatory decision-making on 6 January 2025, built on a seven-step, risk-based credibility framework centred on “Context of Use.”
- The FDA’s CDER has seen more than 500 drug and biologic submissions containing AI components since 2016, concentrated in oncology and neurology.
- In January 2026, the FDA and EMA aligned on shared principles for good AI practice in drug development; India’s CDSCO framework is still evolving, with the DPDP Act, 2023 governing patient data.
- Market forecasts for AI in clinical trials range from about USD 2.75 billion by 2030 (MarketsandMarkets) to about USD 8.5 billion by 2030 (Beroe) — the figures disagree because definitions differ, but all point to fast growth.
- Generative AI can hallucinate — produce confident, fabricated text and citations — which is why no serious organisation lets it write regulatory documents unsupervised.
- For 2026, AI augments clinical-research professionals rather than replacing them; the career advantage goes to people who can use AI tools and judge their output.
If you want to go deeper, the linked articles in this series each take one application apart in detail. And if you would rather talk it through with a person, a counsellor at IICRS is available on WhatsApp.